TRAINING SERVICE PROVIDERS TO SUPPORT AUTISTIC INDIVIDUALS
Section 3: Tailored CSE to the specific needs of ASD individuals
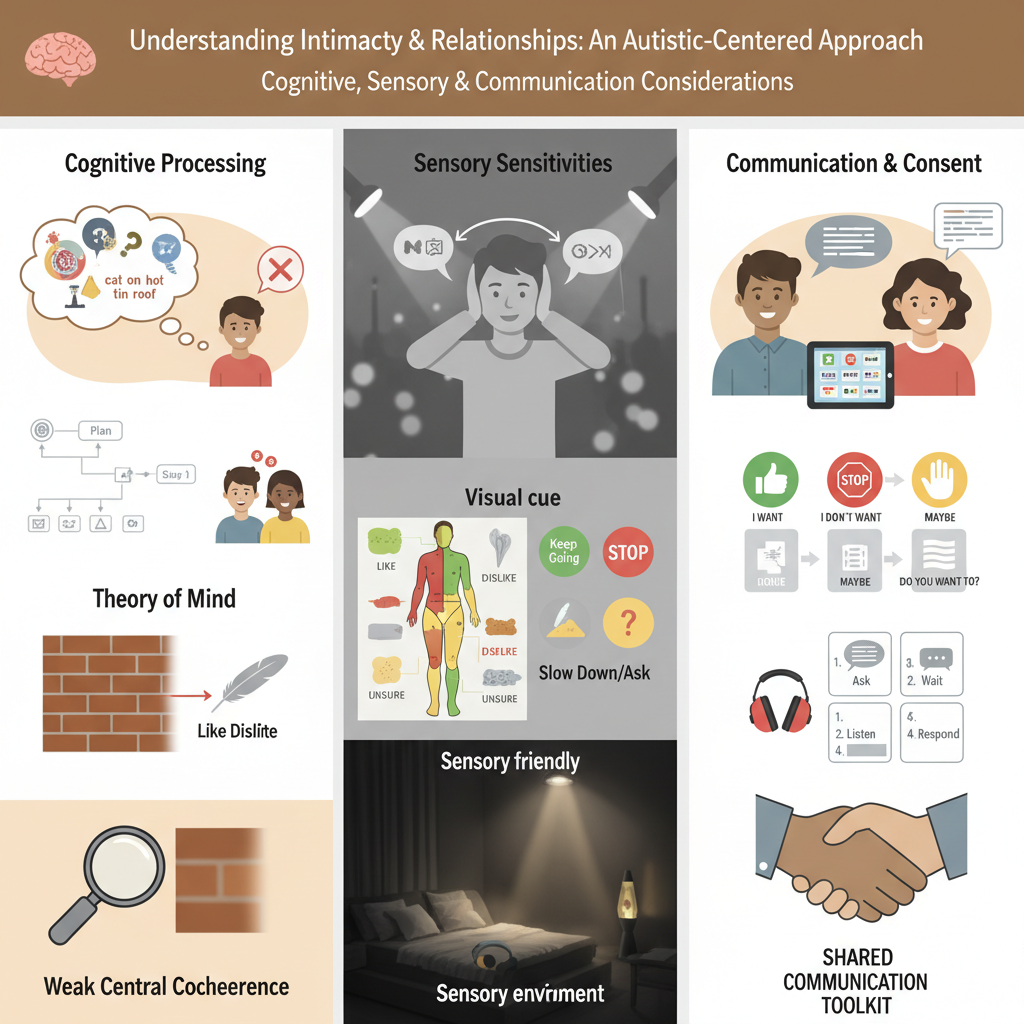
Cognitive, sensory, and communication considerations
Autistic individuals may experience cognitive, sensory, and communication differences that shape how they understand intimacy, relationships, sexuality, and consent. Service providers should offer comprehensive sexuality education (CSE) that is clear, respectful, accessible, and empowering.
Cognitive processing differences
To better understand individuals with autism, it is essential to be familiar with cognitive theories. Cognitive theories can help develop a deeper understanding of how an individual with autism or with related support needs experiences the world and responds accordingly. The theories overlap and are not mutually exclusive; however, each makes a valuable contribution to understanding people with autism (Silberman, 2015).
● Theory of Mind: Differences in understanding others’ perspectives and а non-literal communication (e.g., sarcasm, flirting) can lead to misunderstandings (Fletcher-Watson et al., 2014; Holt et al., 2021).
● Executive function: Difficulties with planning, sequencing, shifting attention, and working memory can affect learning and daily routines (Meltzer, 2018).
● Weak central coherence: Tendency to focus on details over the “big picture,” affecting contextual understanding (Happé & Frith, 2006).
● Context blindness: Difficulty using situational cues in real time, leading to overly literal interpretations and challenges adapting rules across settings (Vermeulen, 2015).
● Double empathy problem: Miscommunication is mutual – non-autistic people may also misunderstand autistic communication (Milton, 2017).
● Monotropism: Strong “attention tunnel,” preference for sameness, difficulty switching tasks, and getting stuck; can affect flexibility and learning (Murray et al., 2005).
Autistic people may also have higher rates of co-occurring conditions (e.g., sleep, GI, anxiety, ADHD), which can influence learning and well-being (Volkmar, 2021). Service providers should therefore prioritise clear, concrete language and support learning with visual support or social stories.
Practical strategies for service providers
Use clear, literal language:
Avoid idioms, metaphors, sarcasm, and euphemisms, which may cause confusion and use direct, concrete terminology instead (American Psychiatric Association, 2013; Attwood, 2007). Repeating key messages in consistent wording and providing step-by-step explanations helps reduce misunderstanding and anxiety (Silberman, 2015).
Use visual and structured supports:
Use visual schedules, diagrams, flow charts, social stories, consent cue cards, and concrete role-plays to reinforce learning (Gray, 2010; Nichols & Blakeley-Smith, 2009). Structured role-play scenarios allow learners to safely rehearse social and sexual communication and support generalisation of skills (Holt et al., 2021).
Support perspective-taking (Theory of mind):
Explicitly teach perspective-taking using scenarios that illustrate different viewpoints and highlight how others may think, feel, or react differently in relationships (Fletcher-Watson et al., 2014). Video modelling and peer mentoring can further support understanding of non-literal language such as sarcasm, jokes, or flirting.
Support executive functioning:
Break tasks into sequenced steps using task analysis (e.g., initiating a conversation, asking someone on a date, or practising safe sex) and provide reminders and structured checklists for daily routines (Meltzer, 2018). Allowing additional processing time can reduce anxiety and increase confidence during social or intimate interactions.
Teach context explicitly (weak central coherence and context blindness):
Help individuals connect specific details to the broader context of health, consent, and mutual respect, rather than focusing only on isolated steps (Happé & Frith, 2006; Vermeulen, 2015). Practising skills across multiple settings supports generalisation and reduces over-literal interpretations.
Address the double empathy problem:
Train both autistic and neurotypical peers or staff in mutual communication strategies, emphasising that miscommunication is reciprocal and not solely the autistic person’s “deficit” (Milton, 2017). Co-creating communication rules within relationships promotes respect, balance, and shared responsibility.
Work with monotropism:
Use strong interests to introduce sexuality and relationship topics and provide warnings for transitions between activities, topics, or routines (Murray et al., 2005). Building on focused interests supports engagement while gradually increasing flexibility and awareness of personal boundaries.
Sensory Sensitivities and Sexuality
Sensory processing differences can strongly affect comfort with touch, noise, smells, and environments during intimacy. Sensory needs vary across people and can change over time. Sexual well-being improves when individuals can recognise and communicate what feels comfortable and what does not (Kirby et al., 2015; Byers et al., 2013). Consent should include sensory boundaries, not only agreement to sexual activity. Behaviours sometimes labelled “inappropriate” may reflect unmet sensory needs rather than intentional rule-breaking (Kapp et al., 2019).
Practical strategies for service providers
Normalise sensory conversations:
Introduce sensory discussions as part of routine sexuality education (e.g., “What kind of touch feels good or not good for you?”). This reduces stigma and builds comfort around expressing sensory needs (Nichols & Blakeley-Smith, 2009). Use simple question cards or worksheets to prompt reflection on sensory likes and dislikes.
Teach consent through sensory boundaries:
Expand the concept of consent to include sensory input. Encourage phrases like “I like firm pressure” or “Stop when I say stop.” Consent is not only about sexual acts but also about respecting comfort zones (Byers, Nichols, & Voyer, 2013). Create visual cue cards (e.g., green = “keep going,” red = “stop,” yellow = “slow down/ask”).
Use visual tools:
Provide body maps for learners to colour or mark the areas of the body they like, dislike, or are unsure about being touched. This supports communication, especially for those with limited verbal expression (Kirby, Dickie, & Baranek, 2015). Additionally, educators can use sensory preference scales with images of textures, sounds, and touch types (light touch, deep pressure).
Create sensory-friendly environments:
Adapt the teaching or therapeutic space to support comfort and focus. This can include dimming harsh lighting, minimising background noise, avoiding strong scents, and maintaining predictable routines. Sensory-safe environments help reduce anxiety and create conditions where learners can engage more openly (Robertson & Simmons, 2015). You can use a sensory environment checklist to regularly assess how classroom or therapy settings meet learners’ sensory needs.
Teach graded exposure and flexibility:
Introduce new sensory experiences gradually, beginning with what the learner already finds comfortable and allowing them to set the pace. This approach builds tolerance and confidence while ensuring that the learner remains in control throughout the process. Graded exposure can reduce avoidance and anxiety, fostering positive and safe associations with physical closeness and intimacy (Crane, Goddard, & Pring, 2009).
Reframe “problematic” behaviours:
When behaviours such as self-stimulation or withdrawal occur, analyse them as responses to sensory needs rather than “misbehaviour.” Pathologising sensory behaviours increases shame; reframing builds understanding and dignity (Kapp et al., 2019). You can develop reflection sheets for staff: For example, “What sensory need might this behaviour be meeting?”
Educate and involve partners:
Encourage partners to ask direct questions about preferences and to respect boundaries. Teach them to observe signs of discomfort (e.g., flinching, withdrawal). Shared responsibility creates healthier, more affirming relationships (Garcia & Houston, 2017). You can create partner-training handouts with sample scripts such as “Do you like this?” or “Should I stop?”
Recognise change over time:
Sensory preferences are not fixed, but they can vary across contexts, moods, and environments. Regularly revisiting each learner’s sensory profile helps ensure that activities and discussions about intimacy continue to match their current comfort levels (Byers et al., 2013).
Communication styles, consent, and AAC
Autistic people may communicate through speech, writing, gestures, or Augmentative and Alternative communication (AAC), often preferring direct language and finding subtle cues (tone, facial expressions, body language) harder to interpret (Müller et al., 2008; Tager-Flusberg et al., 2005). This can affect dating, recognising interest, and navigating consent.
Implications for consent
Indirect refusals (pauses, uncertain tone) may be missed; teaching should emphasize explicit, direct questions and answers (e.g., “Do you want me to kiss you?”) and practice affirmative/refusal language (“I want…” / “I don’t want…”) (Kern & Gaylord, 2006; Nichols & Blakeley-Smith, 2009).
AAC (Augmentative and Alternative Communication)
AAC must be fully integrated into sexuality education so people can express needs, desires and boundaries; exclusion increases the risk of misunderstandings and reduces autonomy (Blackstone et al., 2007; Friedman et al., 2019).
Practical strategies for providers:
● Use direct, unambiguous language.
● Teach what indirect cues can mean (with examples).
● Provide visual scripts and role-play supports for conversations.
● Encourage and model AAC use in consent/relationship topics.
● Teach reciprocal skills: how to ask, respond, and check in.
● Support partners/staff to build a shared “communication toolkit.”